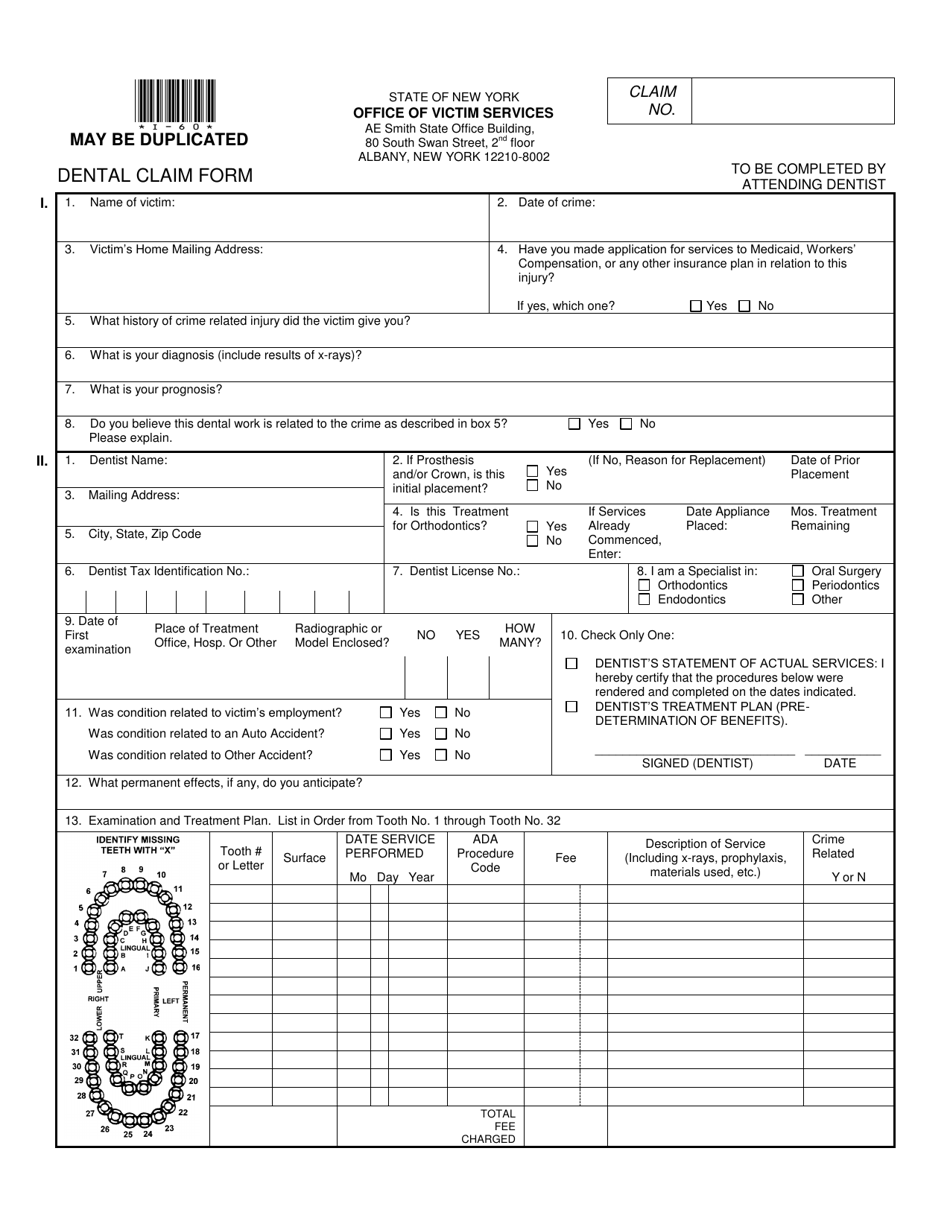
manhattan life dental claim form
VB Accident Claim Form. Submitting THE MANHATTAN LIFE INSURANCE COMPANY Claim Form does.

Manhattan Life Dental Vision And Hearing Plan Youtube
Enter your details to begin.
. VB Life Claim Form. ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Signature Printed Name.
ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Bank Draft Authorization Form In English. By registering and logging in I acknowledge and agree to be bound by the Terms and Conditions for this web site.
VB Cancer Claim Form Printed Name Mail to. 247 patient benefit verification claims and remittance statements. Submit Completed Form to.
Select the appropriate form category to the right. Visit the ContractPolicy Holder. Box 925309 Houston TX 77292-5309 Customer Service.
EASY UPLOAD MOBILE APP. For additional information about dental vision and hearing insurance or any. To process a claim please.
APercentage of Basic eye exam or eye refraction. Signature If Claim Is For A Minor Parent Or Legal Guardian Must Sign Date Submit Completed Form to. The offering Companyies listed below severally or collectively as the content may require are referred to in this authorization as We or ManhattanLife Life.
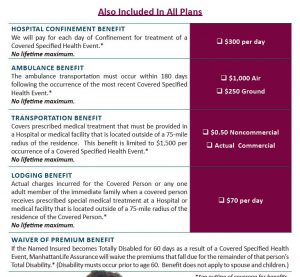
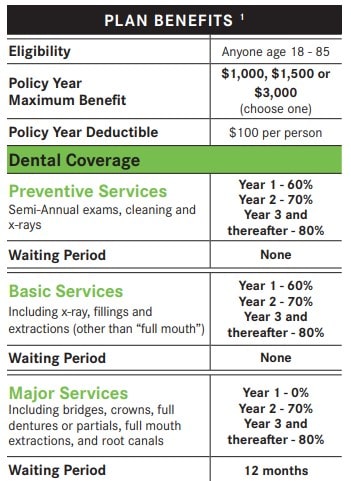
Dental Vision and Hearing insurance from ManhattanLife is designed to meet as many needs outside of standard medical insurance as possible. Life Health Policyholders. Affidavit of Lost Policy - International Life Policies.
Manhattan life dental claim form Monday August 8 2022 Edit. Annuity Cash Value and Maturity Value Request. Report a Death Claim Online Form Acknowledgement of Misplaced Policy.
For Assistance please call1-888-441-07708am - 5pm CST. It provides coverage at the dentist as well. Health Screening Benefit Claim Form ManhattanLife Claims PO.
Or contact our Customer Service department. Benefit exclusions and limitations may apply to the policy. ManhattanLife VB Claims Department PO Box 926169 Houston TX 77292.
The Easy Upload mobile app or the Easy Form Upload tool found on the Client. VB Life Claim Form. Duplicate Policy Request Form.
Dental Vision and Hearing Insurance C-DVH 0615 A plan with choices for you and your family Not available in all. Need to file a Voluntary Benefits Group Policy Claim. Download the filled out form to your gadget by clicking on Done.
For Assistance please call1-888-441-07708am - 5pm CST. Send the electronic form to the parties involved. Select the appropriate form category below.
1-800-669-9030 Annuity Contract Owners.

Illinois Individual Dental Plans

Manhattan Dental Youtube
/Mahattan_life-1fcbe0d5a6e64d97945f758f0d9273b1.jpg)
Manhattan Life Insurance Review 2022

Manhattanlife File A Claim Claim Forms Dental Vision Hearing
Your Best Critical Illness Insurance Options My Family Life Insurance

Blog Dental Vision And Hearing Insurance From Manhattanlife
Bill Downs Insurance Services Llc

Manhattan Life Medicare Supplement Plans For 2022 Medicarefaq
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife

Start A Claim New York Life

Onemanhattandental
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife

Manhattanlife Manhattanlifeco Twitter

Western United Life Medicare Supplement Tidewater Management Group
Here Are 5 Solid Dental Insurance Plans For Seniors On Medicare
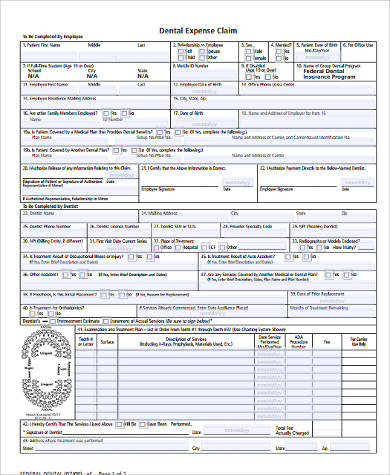
Free 9 Sample Dental Claim Forms In Pdf Ms Word

Manhattanlife Life Insurance Annuity And Supplemental Health Insurance

The Manhattan Life Insurance Company Claim Form Fill And Sign Printable Template Online Us Legal Forms
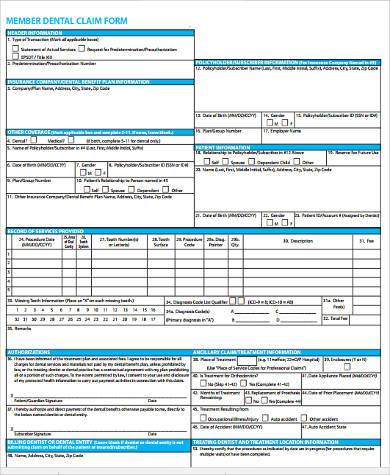
Free 8 Dental Claim Forms Samples In Ms Word Pdf